Common Causes of Vertigo and Imbalance:
Menière's Disease
Menière’s disease is an inner ear disorder whose symptoms are attacks of (non-positional) vertigo with fluctuating hearing and usually tinnitus and aural fullness in the affected ear. It is unusual below the age 40 and can start at any older age. The cause is an abnormal increase in the volume of endolymph in the cochlea, called endolymphatic hydrops. Episodocally the increased endolymph refluxes into the vestibular (otololiths and canals) organs to cause the vertigo attacks.
Usually the first symptom of Menière’s Disease is a severe vertigo attack, accompanied by tinnitus. After the attack there is low tone hearing loss, which may recover. The attacks rarely last longer than 6 hours. As more attacks occur the hearing progressively drops to about 60 dB. An increase in tinnitus and aural fullness can precede an attack. Occasionally the hearing loss may precede the first vertigo attack by months or years.
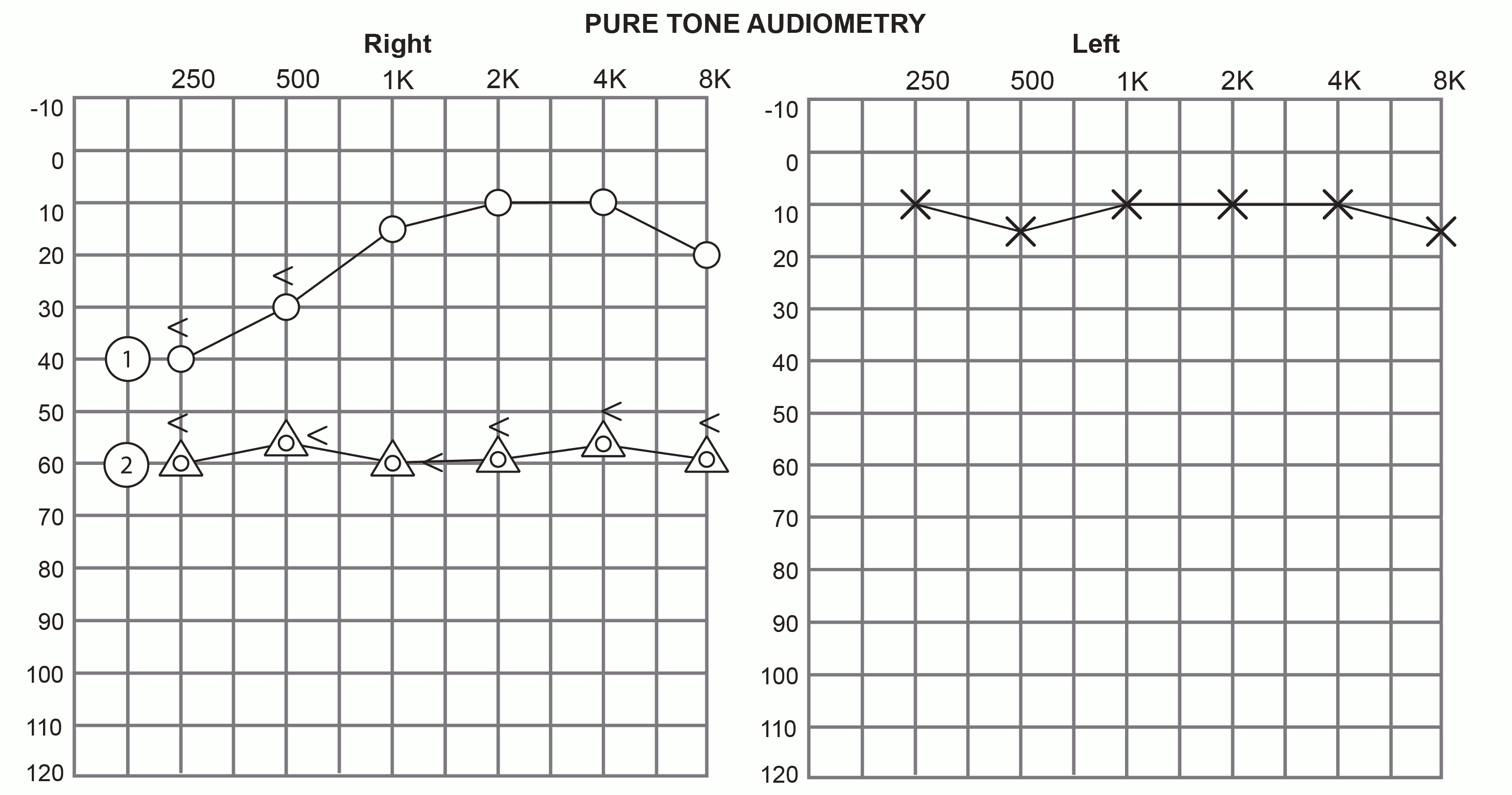
Pure-tone audiogram: Menière's Disease.
In the figure below, the results for the left ear shows hearing within normal limits. The right ear shows two sets of results:
- The initial low-frequency hearing loss.
- The progression of the hearing loss.
The current symptomatic definition of Menière’s disease is by consensus of the Barany Society, the Equilibrium Committee of the American Academy of Otolaryngology-Head and Neck Surgery and the Japan Equilibrium Research Society:
- Two or more spontaneous episodes of vertigo, each lasting 20 minutes to 12 hours;
- Audiometrically documented low-to-medium frequency sensorineural heaing loss on at least one occasion before, during or after one of the episodes of vertigo;
- Fluctuating aural symptoms (hearing, tinnitus or fullness) in the affected ear.
- an MRI scan to rule out an abnormality of the acoustic/vestibular nerve;
- some departments offer an audiological test (tone burst electrocochleography) to confirm endolymphatic hydrops.
Contrary to popular belief there is no evidence that tea, coffee and smoking are a cause. An excess in take of salt as an attack trigger has evidence. There is no evidence that most of the medications which have been used have any effect on preventing attacks or on the course of the disorder. The only oral medication with accepted efficacy is the vasodilator Betahistine. Betahistine is usually commenced at 48mg a day, and can be increased to 96mg a day.
On-going vertigo attacks can be frightening and disruptive and cause significant anxiety in sufferers. If oral therapy is ineffective the options are:
- instillation of gentamycin into the ear as an office treatment;
- inner ear surgery.
Menière’s disease can be difficult to distinguish from Vestibular Migraine.
- Assoc. Prof. Cynthia Darlington